
The Value of Multiplex Staining in the Diagnosis of Cancer



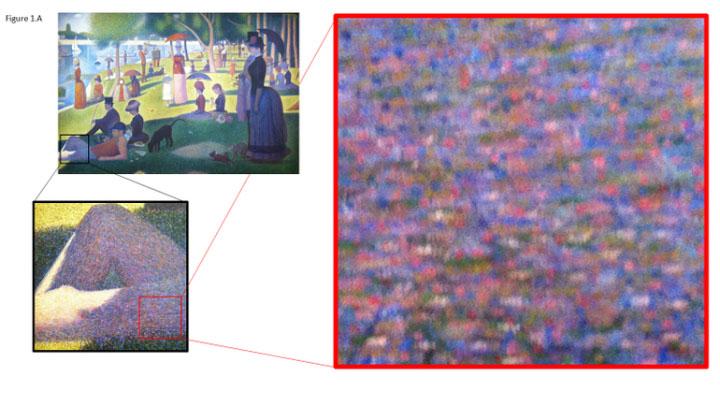
Entering the gallery, you glimpse the wall-sized oil painting, forty paces distant. Green lawn, blue lake, a white sailboat. Approaching, you see people relaxing on the bank, moderate social distancing, enjoying a gentle summer day. You are swept in by Seurat’s masterpiece of Pointillism, A Sunday Afternoon on the Island of La Grande Jatte. Closer examination of the canvas reveals a myriad of tiny dots, each a subtly different color, hue, or shade (Figure 1A). Though famed photographer Ansel Adams might disagree, Seurat’s canvas would not convey its meaning, or be the masterpiece it is, if it were monoplex, composed of only one color.
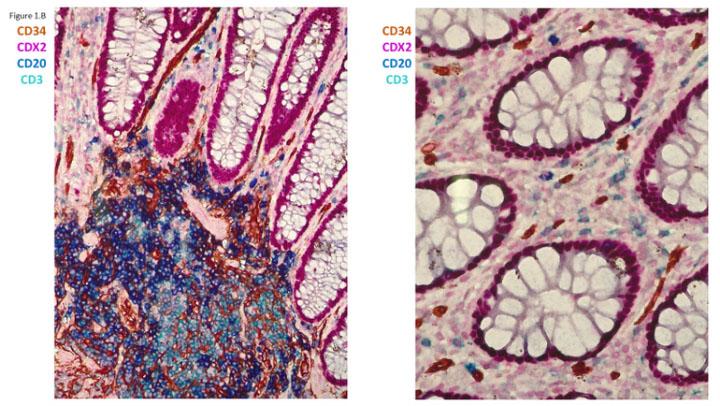
Like the artist, a pathologist often needs to “paint” particular cells or tissues with color to ascertain a cancer diagnosis, but you may be surprised to learn that, unlike the artist, pathologists today predominantly use only one color at a time. Advances in technology now allow the tumor to be painted with multiple colors, termed multiplex staining. An example of four-color multiplex labeling illustrating four different cell types in the human colon is shown in Figure 1B. The purpose of this essay is to describe the process of cancer diagnosis and illustrate why multiplex staining will be integral to cancer diagnoses in the future.
In 2018, 18 million of the Earth’s 7.6 billion people are diagnosed with cancer1. It starts insidiously, years before diagnosis, with one of your body’s 30 trillion cells2 undergoing a mutation, a change in DNA sequence, that allows it to grow, unchecked. More mutations, more growth; months to years pass until one day it grows to become a tumor, at which time it can be seen, felt, or cause symptoms. When the tumor reaches the size of a sugar cube, the single mutated cell has already grown to tens of millions of cells. How then is the tumor diagnosed?
Cancer Diagnosis from a Tissue Biopsy
Although cancers that arise from each body site share features, no two tumors are alike. The diagnosis of cancer today, much like a hundred years ago, requires careful observation of cell and tissue morphology in each tumor. The first step is to collect a biopsy, a piece of the tumor tissue, so that a pathologist can look at the cells with a microscope. The biopsy can range from a very small collection of tissue obtained with a needle, to very large mass excised as a result of major surgery. Diagnosing the tumor as cancer, and which type, is not as simple as the pathologist looking at the biopsy; the tissue must undergo hundreds of individual steps before it reaches the microscope. Early on, the tissue is chemically “fixed” in formalin in order to preserve its structure. This fixed tissue is then embedded in a paraffin wax matrix to allow simplified handling, storage and processing. The tissue is then sliced into razor-thin sections and mounted on glass slides, which can then be stained (“painted”) to illustrate features or specific molecules in the cells and tissues.
The first of these stains is usually with the dyes hematoxylin and eosin (H&E), originally used in the textile industry. The H&E is a 2-color stain that highlights overall cellular architecture, and is the worldwide standard for tissue diagnosis. The pathologist’s impression of the H&E stain then determines which additional stains might be needed to arrive at a diagnosis. Is it a carcinoma, a tumor of epithelial cells, or a lymphoma, a tumor of lymphoid cells? “Special” histochemical stains also use textile dyes, but the major types of modern stains use molecular probes to identify and label specific molecular species in tissue: immunohistochemistry (IHC) uses antibodies to identify proteins or carbohydrates, whereas in situ hybridization (ISH) uses nucleic acids to identify complementary nucleic acids (DNA or RNA).
A cancer diagnosis in 2020 typically includes several molecular stains to establish the exact tumor type. Additional stains may be required for a complete diagnosis including a second opinion, informing prognosis, and predicting which targeted therapies might give the patient the longest life or best chance of survival. For many reasons, including the 3Rs – rapidity, robustness, and reimbursement – the vast majority of additional stains are monoplex, done by applying a single probe to a separate section (slice) of tissue and using a single color to visualize its distribution in tissue. For complex cases the total number of stains can exceed two dozen, each requiring a separate tissue section. Though tissue sections are thin, using this many of them can be wasteful, especially if tissue is needed for other diagnostic tests. The pathologist must then integrate each of these single stains in their brain, to create a multicolor image of the patient’s tumor.
Multiplex Staining: The Next Dimension of Cancer Diagnosis
Today, multiplex staining is frequently performed in research in order to gain deeper insight into tissue samples, but due to a combination of technical, operational, and financial factors it is rarely performed in clinical diagnostic labs as part of cancer diagnosis. Multiplex offers multiple potential advantages for arriving at cancer diagnoses including:
- Preservation of tissue. Lung cancer diagnosis and therapies have undergone rapid advancement in the past decade, but most lung cancer patients are unable to undergo surgery when they present with cancer. For these reasons, lung cancer is often diagnosed with a needle biopsy, which generates a very tiny sample. As of mid-2020 there are nine different molecular abnormalities in lung cancer linked to targeted therapies, each requiring a separate test that consumes a separate slice of tissue. In addition, some of the tests require sending several slices of tissue to a large reference lab or core facility to perform next generation sequencing (NGS). Adoption of multiplex staining for lung cancer diagnosis could help preserve tissue to ensure an accurate diagnosis is made without the need to re-biopsy the patient.
- Improved diagnostic accuracy. Diagnosis of prostate cancer typically involves examination of over a dozen needle biopsies, and the patient’s diagnosis and choice of therapy depends critically on identifying the type, extent, and size of cancer throughout the biopsies. While some prostate cancer cells are easy to recognize in a biopsy, others may masquerade as benign cells. A multiplex stain called PIN4 combines markers in benign and malignant prostate cells so that both types of cells can be seen in the same section using different colors, helping the pathologist make the diagnosis of prostate cancer (or rule it out) more confidently.
- Enhanced diagnostic insight. As we learn more about how tumors grow and how new therapies can prevent their growth, multiplexing will be an essential technique to visualize these factors in each tumor. For example, a new generation of medicines, the immune checkpoint inhibitors, block the ability of the tumor to prevent the patient’s immune system from fighting the tumor. While much remains to be learned, it is increasingly recognized that features of various immune cells in the tumor, including their location and activation state, influence how checkpoint inhibitors work. For example, the lymphocytes in a tumor can be in states of “activation” or “exhaustion”, each of which can be visualized in each cell by expression of different proteins painted in different colors. Tumors often recruit non-tumor cells called myeloid derived suppressor cells (MDSCs) that locally shut down the anti-tumor immune response. Finally, much has been studied about how different populations of macrophages, the body’s scavenger cells, can be pro- or anti-inflammatory and thus play opposite roles in tumor growth. While these two functions have been attributed to two types of macrophages, designated M1 or M2, recent observations suggest there not two but rather nine different types of macrophages in the body! At present, none of these observations are used in routine diagnosis of cancer patients because they have not yet been shown to influence prognosis or therapy selection, but emerging research tells us they are incredibly important. Knowledge is accumulating rapidly, so it is only a matter of time until diagnostic tests will include tumor immune infiltrate assessments, which will likely require multiplex staining.
Consider the simplicity of the current monoplex approach to cancer diagnosis in relation to the sheer complexity of cancer tissue. Indeed, the complexity of a single cell, which measures a mere 1/100 of a millimeter in diameter, is staggering. Each normal human cell contains about two yards of DNA, three billion base pairs, that encode ~21,000 genes, each of which can make many different RNAs. In a typical cell at any given time are more than a million RNAs that have directed the synthesis of million protein molecules. The proteins are the cell’s building blocks and components of the tiny, macromolecular machines that run the factory that is each cell. Cancer is a disease of DNA; changes in DNA cause changes in proteins that alter the cell’s structure as well as function of many of the little machines in the tumor cells that result in unchecked growth of the tumor.
Cancer cells exhibit far more abnormalities, complexity, and heterogeneity than non-cancer cells. Yet, in 2020 for cancer diagnosis we still examine only one type of molecule (nucleic acid or protein) in each tissue section at a time! Emerging research techniques involving detection of markers with fluorescence or mass spectrometry can increase the number of observable molecules at a time by tenfold over traditional techniques, and an emerging technique termed single cell analysis can quantify thousands of different molecules in each cell. The amount of data that can be extracted from one tumor is enormous, yet most of it is extraneous to the patient’s diagnosis. Pathologists believe that it is important to observe molecules in tissue sections in order to make the best diagnosis. Multiplexing can solve the problem of visualizing the right set of molecules in each patient’s tissue section. The challenge will be to only measure the molecules that will give the cancer patient the best chance of a longer life or a cure.
Challenges Associated with Multiplexing in the Clinical Setting
Multiplex staining is not without barriers to implementation in clinical care, including the need for extensive test validation, increased test run time, the cost of reagents compared to an equivalent number of monoplex stains, and a scarcity of technicians skilled to run and interpret tests. Validation of a multiplex test must include comparisons with the panel of monoplex tests that comprise it, meaning not only increased validation requirements but also the need for digital and computational solutions to remove bias and error. While monoplex IHC and ISH tests were first performed manually, the advent of automated robotic stainers in the 1990s reduced test turnaround time while improving reproducibility. Current automated multiplex stain protocols still typically take longer than their monoplex equivalents. Reagent cost remains an issue, although we anticipate wider adoption will reduce costs in the long run. Finally, limited reimbursement options exist for multiplex tissue testing. Current fee schedules assume only cost savings, if any, gained by multiplexing, while ignoring the increased time needed for more complex analysis, and, importantly, potential added value to the patient.
Will the promise of multiplexing be realized by digital pathology?
There are also challenges around test interpretation that increase with the number of markers measured at a time. Because pathologists are used to interpreting monoplex stains that generally label one cell type or tissue compartment, interpretation of a duplex (two markers) or triplex (three markers) stain is generally not more difficult than interpreting a set of monoplex stains if each stain labels different (not overlapping) areas of the tissue section. Indeed, in many circumstances (such as PIN4 above) there is added value in simultaneous observation of two or more markers in the same section. However, if two or more molecules are present in the same cell compartment or tissue, and the quantity of the molecule in the cell is important to assess its status (e.g. absent vs. present, and if so, high vs. low levels), even the best pathologist’s eyes and brain are not up to the task. Now imagine visualizing 30 or 3000 molecules per cell! Clearly, computer programs that help analyze the images are required for interpretation. Fortunately, we are rapidly entering the age of “digital pathology” in which interpretation of patient tissues will soon be more likely to occur on a computer screen than by traditional microscope. With adoption of digital pathology will come “apps” including molecule quantitation and artificial intelligence that will help the pathologist interpret the complex datasets that multiplex stains can generate.
The Future of Multiplexing
Advances in cancer treatment are increasingly linked to specific molecular abnormalities in each patient’s cancer, which has led to increased complexity of each patient’s biopsy workup. As the number of molecules requiring interrogation in cancer biopsies continues to rise, we believe multiplexing will play a greater role in biopsy analysis by maximizing use of limited tissue, improving diagnostic accuracy, and enhancing diagnostic insight, as well as serving as a better predictor of prognosis and guide the selection of therapy. In addition to advancements in staining technology, full adoption of multiplex will require digital, computational, and ultimately artificial intelligence tools to support increasingly individualized diagnoses and personalized therapies. Just as the practice of medicine remains an equal mix of art and science, the pathologists' interpretation of molecules in tissue will create a vibrant portrait of cancer tissue that enables precision treatments and improved outcomes for cancer patients.
About the presenters
Keith Wharton has 30+ years of experience in academic and biopharma settings, including Leica Biosystems, Novartis, and Biogen. Following board certification in anatomic pathology and fellowship training in autopsy pathology and developmental biology at Stanford University, he ran an NIH-funded research laboratory at UT Southwestern Medical Center and held several leadership positions including Pathology course director, Director of the Laboratory of Molecular Pathology, and Associate Dean.
Jonathan Roy Vice President of Pharma Partnerships, Jon is leading Companion Diagnostic development for Leica Biosystems. He has spent the last 10 years focused on companion diagnostic development and implementation globally both at Leica and as Head of Commercial Strategy for Companion Diagnostics at GlaxoSmithKline.
Kimberly Byrwa-Neff is a registered nurse with a background in both clinical nursing and in evidence generation in industry. Her clinical expertise lies in cardiology and oncology, specifically breast cancer. As a nurse, black belt in process excellence, daughter of a breast cancer patient, and survivor of breast cancer herself she brings the full patient experience to her work to improve care for breast cancer patients. Kimberly has authored numerous papers and presented improvement in clinical outcomes as a result of working with breast teams across the country.
Referenzen
1. Globocan 2018, World Health Organization, IARC Retrieved from 900 World Fact Sheet The Global Cancer Observatory May, 2019. Retrieved from https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.21492
2. Sender, R., et.al., PLOS Biology, Revised Estimates for the Number of Human and Bacterial Cells in the Body; Aug. 19, 2016 Retrieved from: https://journals.plos.org/plosbiology...
Related Content



Die Inhalte des Knowledge Pathway von Leica Biosystems unterliegen den Nutzungsbedingungen der Website von Leica Biosystems, die hier eingesehen werden können: Rechtlicher Hinweis. Der Inhalt, einschließlich der Webinare, Schulungspräsentationen und ähnlicher Materialien, soll allgemeine Informationen zu bestimmten Themen liefern, die für medizinische Fachkräfte von Interesse sind. Er soll explizit nicht der medizinischen, behördlichen oder rechtlichen Beratung dienen und kann diese auch nicht ersetzen. Die Ansichten und Meinungen, die in Inhalten Dritter zum Ausdruck gebracht werden, spiegeln die persönlichen Auffassungen der Sprecher/Autoren wider und decken sich nicht notwendigerweise mit denen von Leica Biosystems, seinen Mitarbeitern oder Vertretern. Jegliche in den Inhalten enthaltene Links, die auf Quellen oder Inhalte Dritter verweisen, werden lediglich aus Gründen Ihrer Annehmlichkeit zur Verfügung gestellt.
Vor dem Gebrauch sollten die Produktinformationen, Beilagen und Bedienungsanleitungen der jeweiligen Medikamente und Geräte konsultiert werden.
Copyright © 2026 Leica Biosystems division of Leica Microsystems, Inc. and its Leica Biosystems affiliates. All rights reserved. LEICA and the Leica Logo are registered trademarks of Leica Microsystems IR GmbH.