
Specimen Tracking Systems: Tracking Samples Helps Reduce Misdiagnosis

Every year, around seven billion samples are tested in US laboratories alone. It is a critical part of the diagnostic process, contributing to 70 percent of all medical decisions that are made. Alarmingly, it is estimated that up to 98,0001 people die in hospitals each year from preventable medical errors, making misdiagnosis the eighth leading cause of death in the US, ahead of motor vehicle accidents, breast cancer and AIDS.
One of the most common and preventable causes leading to misdiagnosis comes from a surprisingly simple step in the process – the labeling of tissue samples.
Preparing tissue for diagnosis

To diagnose medical conditions such as cancer, a tissue sample is taken from the patient for testing. This sample is cut-up and placed into laboratory cassettes. From there, the sample is embedded in paraffin so it can be cut into even thinner sections and placed onto slides. The sample is stained using various techniques that enable a pathologist to visualize the tissue using a microscope and make a diagnosis. The result is then sent back to the treating physician who discusses the results and treatment options with the patient.
What is sample tracking?
Sample tracking helps laboratories know where samples are in the testing process. If additional tests are ordered, sample tracking allows the laboratory to rapidly identify the patient information and any previous testing carried out on the sample.
Some laboratories create a manual log of where the sample has been and who has touched it. For others, digital tracking solutions create this log automatically. Laboratories that rely on manually handwriting logs not only tie up technicians for longer periods of time, they also face the increased risk of errors being made.
Misdiagnosis through patient identification errors

No matter how accurate the diagnosis is, if it is not matched to the correct patient, it is worth nothing. Errors can lead to added patient stress around further testing, increased medical costs, delays in treatment and in the worst cases, the wrong treatment – or no treatment at all.
Of course, not all errors are caused by the mislabeling of samples. There can be many reasons for a lab error, from mishandling samples to slide contamination. However, incorrect sample labeling is still a significant contributor to patient misdiagnosis. Patient identification errors in anatomic pathology have been estimated to occur in around four out of every 1000 surgical specimens2. Approximately two in every 1000 medical reports don’t go to the right patient3 and one in every 1000 cases are affected by mislabeling.
When it comes to mislabeling sample tests, an error rate of 0.1 percent may seem relatively small. However, when weighed up against the 7.6 billion sample tests performed in the US alone each year, the numbers surrounding misdiagnosis are uncomfortable at the least.
In 2006, a 69-year-old woman in Japan had her left thyroid gland mistakenly removed after her sample was confused with that of another patient with thyroid cancer. In 2009, a woman in the US was told she did not have breast cancer eight days after having a mastectomy. Her doctor told her that her slides had been mixed up with those of another patient at the laboratory. Similarly, in 2010, another woman in the US had a double mastectomy after a mislabeled sample tissue led doctors to incorrectly diagnose an invasive form of breast cancer. The patient even sought the second opinion of another doctor before the operation. Unfortunately, the second doctor relied on the same mislabeled sample as the first, so her efforts were in vain.
Sadly, the stories go on. It is no wonder that legal cases in the US around the cancer misdiagnosis are increasing.
Why are sample labeling errors being made?
Some believe such mistakes happen because of bad processes, or because there are not enough checks for errors made by laboratories. While this may be the case in some instances, most laboratories operate with the greatest of care, going to extreme lengths to check details over and over.
Every laboratory in the world must be able to produce, collect, interpret, share and store data, matching the results of the testing to a patient’s details (name, address, age, doctor etc.). There may be as many as eight separate steps in the testing process – even more if the sample requires secondary testing.
One of the problems leading to mislabeling is the sheer volume of testing carried out by laboratories, struggling to keep up with the demand for rapid results from an increasing number of patients. As the population ages, the number of cancer cases are on the rise. The workload laboratory technicians’ face is increasing year on year. At the same time, technicians are under mounting pressure to reduce the time to diagnosis in order to treat aggressive cancers in time.
Funding for the industry is also at an all time low. This, coupled with a labor shortage means existing laboratory technicians must simply manage doing more, with less. Under time and space constraints, even the most vigilant laboratory technician can make mistakes.
The challenges of manual sample tracking

When it comes to filling out, verifying and logging a patient’s details, there are multiple potential points of error in a laboratory’s process. One is the reliance on handwriting, where interpreting a faded label or illegible handwriting can all-too-easily result in mistakes. When reading a handwritten label, it is understandable how a ‘5’ may in some instances be mistaken for an ‘S’. Similarly, a ‘1’ might be mistaken for a ‘7’, or perhaps an ‘l’. Some laboratory technicians responsible for reading, interpreting and relabeling patient slides have even been known as sufferers of dyslexia, adding further hurdles to the process.
When sample tracking is performed manually, laboratories will commonly sort slides and cassettes into the different testing phases so that the same procedure can be performed on multiple samples at the one time. The slides are then resorted according to patient. However, handling slides in batches introduces the risk that the slides may be matched to the wrong block.
Another risk comes from re-labeling slides. Usually, the laboratory will need to re-label slides at certain stages in the process. Every time a slide must be relabeled, it introduces the possibility of error.
Keying in data into a computer can also present risks. The Ohio University Center for Automatic Identification found that even a well-trained data entry operator makes a data entry error one in every 300 keystrokes.
It is still not a 100% exact science determining whether a person has cancer from a slide. It requires great experience, and in difficult cases, second and third opinions. Still, no matter how careful a laboratory technician is, the risk of human error is always present. When it comes to capturing critical patient information multiple times a day, it is inevitable that along the line, mistakes will be made.
What can be done to reduce misdiagnosis?
Uniquely identifying the sample early in the process and using bar coding and software to identify and track the specimen can significantly reduce the risk of misdiagnosis. A system that can eliminate these errors can provide great relief to not only those working with samples, but most importantly, for the patients concerned.
In the late 1980’s and early 1990’s, medical laboratories began experimenting with the use of barcode identification of tissue specimens. Today, most laboratories use some form of coding during the histology testing process. Most commonly, a number is created to identify a patient, which is then used to track a sample. In many cases however, the same number can’t be tracked throughout the whole process, and the sample must be re-labeled at particular points. Unless a laboratory is using a barcode and scanning together with their data management software throughout, there is still a risk of human error if the information must be re-entered from one system to another.
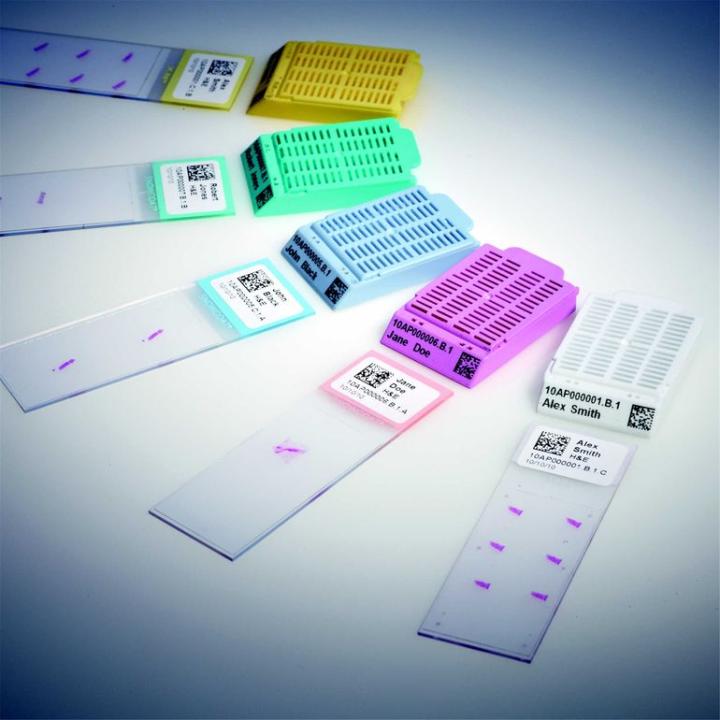
Identification errors can be greatly reduced by labeling slides and cassettes with barcodes. For example, using two dimensional (or 2D) barcodes to mark samples can produce error rates as low as one in 612.9 million scans.
How does barcoded sample tracking work?

With a barcoded tissue tracking solution, laboratories are able to confirm the identity of every container, cassette and slide – matched with the identity of the patient – throughout the complete diagnostic process. For any patient tissue obtained from the operating theater, a unique identifier is assigned and attached to the sample. Barcode readers are then used to track where that sample goes through the different steps of the process.
Each patient has a unique identification number. This number is clearly and permanently printed on each specimen container along with a barcode representing the ID number in scannable form. When the specimen container is scanned, the system automatically prints the required number of cassettes, complete with identifying numbers and barcodes.
If for some reason anyone uses a cassette from another patient, the system will automatically notify them of the error. This error is also recorded into the system log, so that afterwards, the laboratory can investigate how the error was made to prevent future errors and to optimize its processes.
When the tissue is cut to a slide at the sectioning stage, slide labels are printed, each featuring a barcode. The tissue is then placed on the slide and rescanned, making sure it can be accurately plotted to match the patient’s identity. If the slide appeared different, again the system will alert the technician.
The bar coding system ensures that only one patient’s samples are handled at a time to prevent any confusion of slides between patients. Every time a sample is scanned, the laboratory can track its process, where it is and who handled it, providing full traceability.
According to the Department of Pathology University Hospitals Case Medical Center in Cleveland, Ohio, the use of bar coding and tracking in surgical pathology has significantly decreased the hospital’s number of errors from 11-14 slides out of 10,000 to 0-1 out of 10,000.
Another example is at the Henry Ford Hospital in Detroit, Michigan, where a 62% reduction in case misidentification was reported using bar coding. By automating tasks around labeling, laboratory technicians at the hospital have been able to each free up around 12 hours of work per week.
Adopting a ‘Lean’ approach
As workloads increase each year, many laboratories are looking into different process improvement methodologies to optimize their efficiency. One of the methodologies the medical world is currently focused on is adopting a ‘lean’ approach.
A ‘Lean’ histology practice is all about maximizing efficiency, reducing costs, saving time and delivering better patient care. In a nutshell, it’s about finding out what steps in the process add value, what steps do not. Automation, when properly designed, is often an effective way to improve efficiency and reduce waste.
Sample tracking can help with Lean implementation in several ways. Firstly, a sample tracking system can accurately measure process time, so it can be easy to identify delays, and confirm improvements by checking before and after times.
Also, in a troubleshooting situation, a sample tracking can be a powerful tool. For example, if a laboratory technician finds a slide out of place and needs to identify it. With manual log books, the technician would have to search back several days across the different testing phases – a task that could take hours. With barcode technology, the answer is instantaneous.
The future of sample tracking
Today, sample tracking covers all the major steps in the histology testing process. In the future, we can expect to track more detailed steps in the process, dramatically improving the accuracy of diagnostic testing and reducing the possibility of errors by misidentified samples.
While presently laboratories scan barcodes using a hand scanner, the laboratory solution of the future will have inbuilt scanners that can instantly recognize a sample pot or cassette.
There will also be a range of different identification methods available aside from bar coding. One such method being trialed is Radio Frequency Identification, or RFID. With this method, the system recognizes the sample as soon as it comes into close proximity. It is the same system used by supermarkets and retail stores today to prevent shoplifting. Although the technology is already available, it is not yet economically viable for laboratories performing high volume, low cost testing. It is however already being used by laboratories to track expensive instruments and reagents, providing another exciting avenue for improving the granularity in sample tracking and the accuracy of patient diagnosis.
About the presenter
Mikko Rasanen has an M.Sc. from the University of Turku, Finland, with a major in computer science. He has 15 years of experience in various R&D and marketing positions within the medical device manufacturing industry, focusing on creating solutions for population screening, dental x-ray imaging, and anatomical pathology.
References
- ‘To Err is Human’, Institute of Medicine, November 1999
- Makary MA et al. Surgical specimen identification errors…. Surgery 2007 Apr;141(4):450-5
- Nakhleh RE, et al. Amended reports … Q-probes study of 1,667,547 accessioned cases ... Arch Pathol Lab Med. 1998 Apr;122(4):303-9.
Leica Biosystems Knowledge Pathway content is subject to the Leica Biosystems website terms of use, available at: Legal Notice. The content, including webinars, training presentations and related materials is intended to provide general information regarding particular subjects of interest to health care professionals and is not intended to be, and should not be construed as, medical, regulatory or legal advice. The views and opinions expressed in any third-party content reflect the personal views and opinions of the speaker(s)/author(s) and do not necessarily represent or reflect the views or opinions of Leica Biosystems, its employees or agents. Any links contained in the content which provides access to third party resources or content is provided for convenience only.
For the use of any product, the applicable product documentation, including information guides, inserts and operation manuals should be consulted.
Copyright © 2026 Leica Biosystems division of Leica Microsystems, Inc. and its Leica Biosystems affiliates. All rights reserved. LEICA and the Leica Logo are registered trademarks of Leica Microsystems IR GmbH.