
Knife Angle in Microtomy

To prepare biological tissue for observation under a microscope, the tissue is usually cut in thin slices. Most biological tissue is too soft to cut; the knife would push into it and compress it, even if the cutting edge was very sharp. Therefore, the tissue can be frozen and sectioned in a cryostat, embedded in a hardening material like paraffin or resin, or cut while still soft with a vibrating blade microtome. The correct knife angle is the subject of much misunderstanding, misleading experience, and incorrect information passed between microtomists, but in fact, can be logically derived.
Ideal versus compromise
The ideal knife for sectioning any material in any microtome, regardless of specimen hardness, would be an infinitely thin plane. This would be oriented parallel to the plane of the cutting movement. Unfortunately, infinitely thin planes are hard to come by, and in fact, are found only in geometry books.
Real knives are a compromise, or several compromises, between physics, available materials, manufacturability, and cost. They must have measurable thickness to be held stable during cutting. So, the leading edge must be made thinner than the main body of the knife, in a wedge shape, to enable both cutting and physical inflexibility. All microtome knives, whether resharpenable or disposable, have a wedge shaped part.
The entire knife could in theory be a smooth wedge, with gradual slope to the leading edge. However, sharpening the knife would then require removing a layer from at least one whole face of the knife. In practice, there is always a final bevel at a steeper angle for about a millimeter back from the cutting edge. The final bevel may be symmetrical on both sides, or not. The final bevel helps with sharpening and resharpening, only the bevel face(s) surface has to be removed to sharpen.
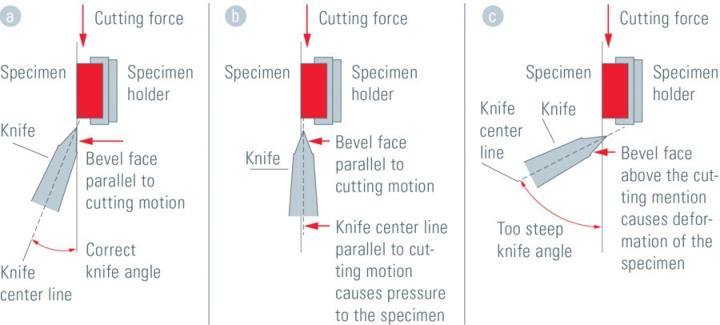
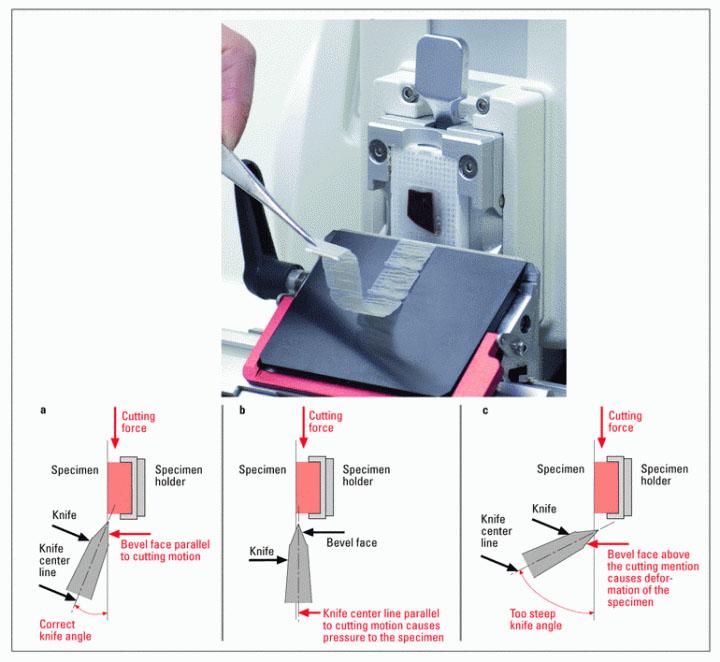
In a microtome, the center line through the cross-section of the knife, as shown in Fig. 1a, is always positioned at an angle to the main direction of motion, not parallel to the direction of motion as it would be for an ideal infinitely thin knife. This is necessary because of the bevel. The angle is required because the knife is wedge shaped in cross-section (at least the beveled leading edge of it). This compromise with the ideal knife has two negative consequences.
Consequences of too shallow an angle
Suppose the knife is held so that the plane of motion (of the knife or specimen) is parallel to the centerline through the wedge, as would be appropriate with an ideal knife (Fig. 1b). The face of the bevel on the specimen side of the knife would then be pressed hard against the specimen, increasingly so with more cutting movement and apply compressive and forward pressure to the specimen. This is never good, and there are several possible consequences that depend on the tissue properties, knife properties, and on how well the specimen is adhered to the specimen holder:
- If the tissue is soft, the section will be cut, but the block face where the next section will come from will be compressed down and forward, abraded, and damaged. The most common result is alternating thick and thin sections (this can also occur if either the knife or the specimen holder is not tightly secured and can move under pressure).
- If the tissue is hard, or a vibrating blade is used (see Fig. 2), the result of the pressure may be not to compress the tissue but to flex the knife upward. If the knife can be flexed, it may “skate” up out of the tissue somewhere in the interior of the intended section, separating partial fragments, or make a wavy pattern on the block surface, called "Venetian blinds", where the knife is deflected up, then springs back. Some degree of waves can happen even with the correct knife angle, due to specimen compression in front of the knife.
- Excessive forward push on the specimen block could cause the specimen to break off the specimen holder.
The lesson here is that the knife always needs a high enough angle to prevent the trailing part of the lower bevel face from applying pressure to the specimen block.

Consequences of too steep an angle
Suppose instead that the knife is raised to a steep angle between a center line through the knife cross section and the axis of movement, so that the lower face of the wedge no longer pushes down and forward on the block (Fig. 1c). However, the upper face of the wedge is always pushing on the uncut specimen above the cutting edge. This bends the section very sharply up at the line of cut as it is separated from the specimen block. As with any object with any thickness being bent, the lower surface of the section at the bend will be stretched, and some separations will occur. The upper surface will be compressed. If the deformed specimen does not spring back, the tissue will roll into a tight roll. Even if it does spring back, and is prevented from rolling, the section will be altered. It is never good to bend the section more that it has to bend given the need to push the wedge in. There are again several possible consequences, depending on the specimen and knife properties:
- If the knife is flexible and the specimen is hard, the knife may bend down and dive into the specimen block.
- If the specimen is hard, it may have shatter, sometimes called "chatter", lines running parallel to the knife edge, where the hard section was sharply bent and broke.
- If the specimen is weakly connected, the section may look more like scrapings than a smooth section.
- A soft section may roll up in a tight roll, taking the shape given it at the line of cut.
What is the correct knife angle?
As a general principle, excessive bending of the section at the cut line is never advantageous in histology or material sectioning. However, errors of too shallow an angle are more damaging to the specimen than errors of too steep an angle. This leads inevitably to the conclusion that the correct knife angle should always be set in the following manner: Position the lower bevel face parallel to the specimen block and the plane of motion. Then raise the angle slightly (1/2 degree if you can manage such a thing) above the bevel angle to avoid having the lower bevel face slide over the specimen block and possibly produce friction damage. The correct knife angle positioning should be consistent regardless of the type of microtome or any specimen property.
The consequences of incorrect knife angle will vary because of differences in specimen types, fixation and processing qualities, and knife flexibility. Knife and disposable blade properties must also be considered because they can be manufactured with different profiles and angles. The correct knife angle is the property of both the knife and its final bevel. These characteristics may vary between manufacturers and may also change after re-sharpening.
About the presenter
Charles Scouten acquired his Ph.D from SUNY Binghamton in 1980 with a dissertation entitled “Location of Neurons Mediating Androgen’s effect on Copulation, Urine Marking, and Body Weight”.
Related Content




Leica Biosystems Knowledge Pathway content is subject to the Leica Biosystems website terms of use, available at: Legal Notice. The content, including webinars, training presentations and related materials is intended to provide general information regarding particular subjects of interest to health care professionals and is not intended to be, and should not be construed as, medical, regulatory or legal advice. The views and opinions expressed in any third-party content reflect the personal views and opinions of the speaker(s)/author(s) and do not necessarily represent or reflect the views or opinions of Leica Biosystems, its employees or agents. Any links contained in the content which provides access to third party resources or content is provided for convenience only.
For the use of any product, the applicable product documentation, including information guides, inserts and operation manuals should be consulted.
Copyright © 2026 Leica Biosystems division of Leica Microsystems, Inc. and its Leica Biosystems affiliates. All rights reserved. LEICA and the Leica Logo are registered trademarks of Leica Microsystems IR GmbH.